REASON 01 — THE PROBLEM
Magnesium can't reach this. Neither can HRT.
The problem isn't in your supplement drawer. It's autonomic.
Perimenopause is the body's slow disconnection from estrogen. That sounds hormonal — and it is — but the symptom you wake up to isn't a hormone shortage. It's a broken handoff between your sympathetic ("fight or flight") and parasympathetic ("rest and digest") nervous systems.
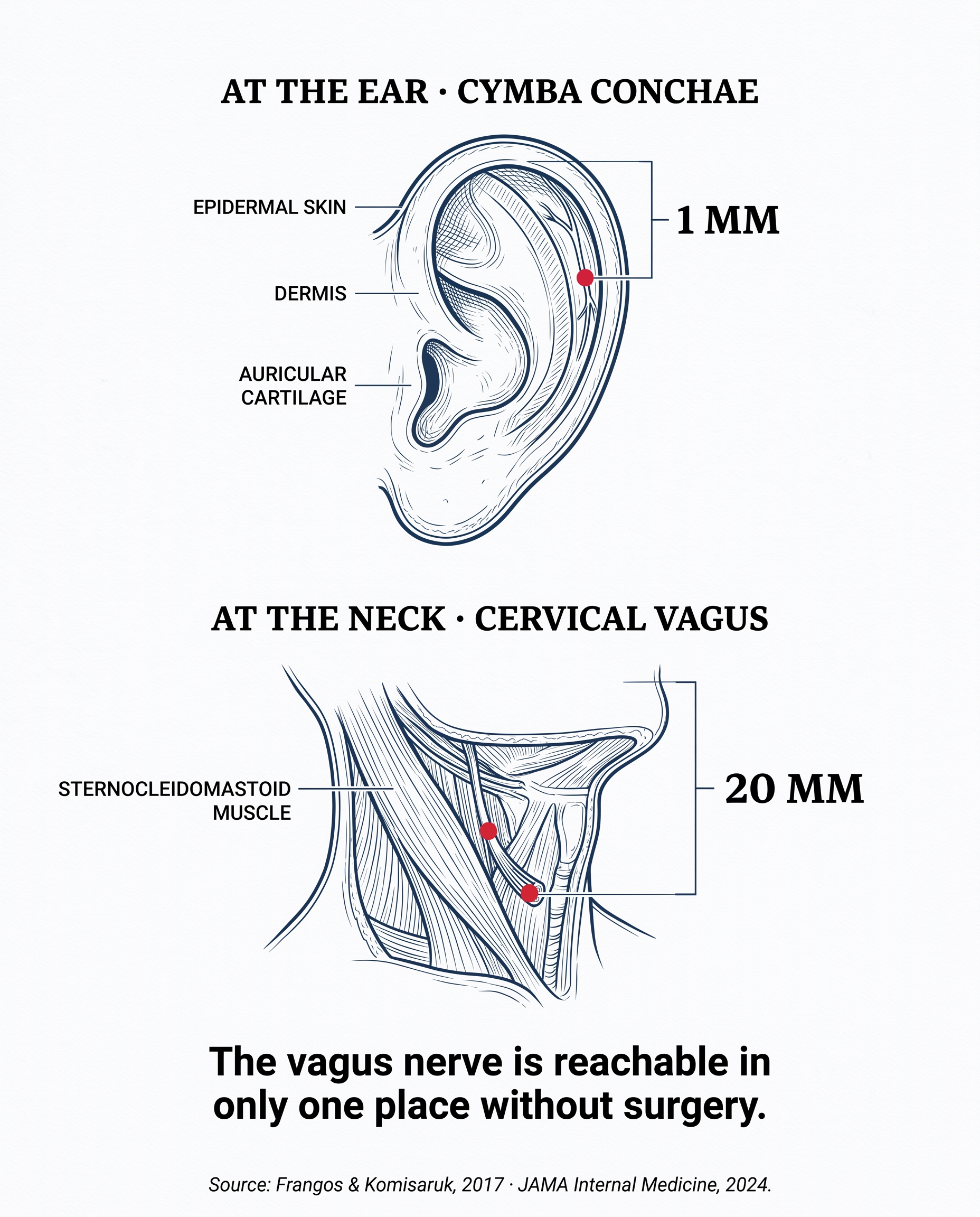
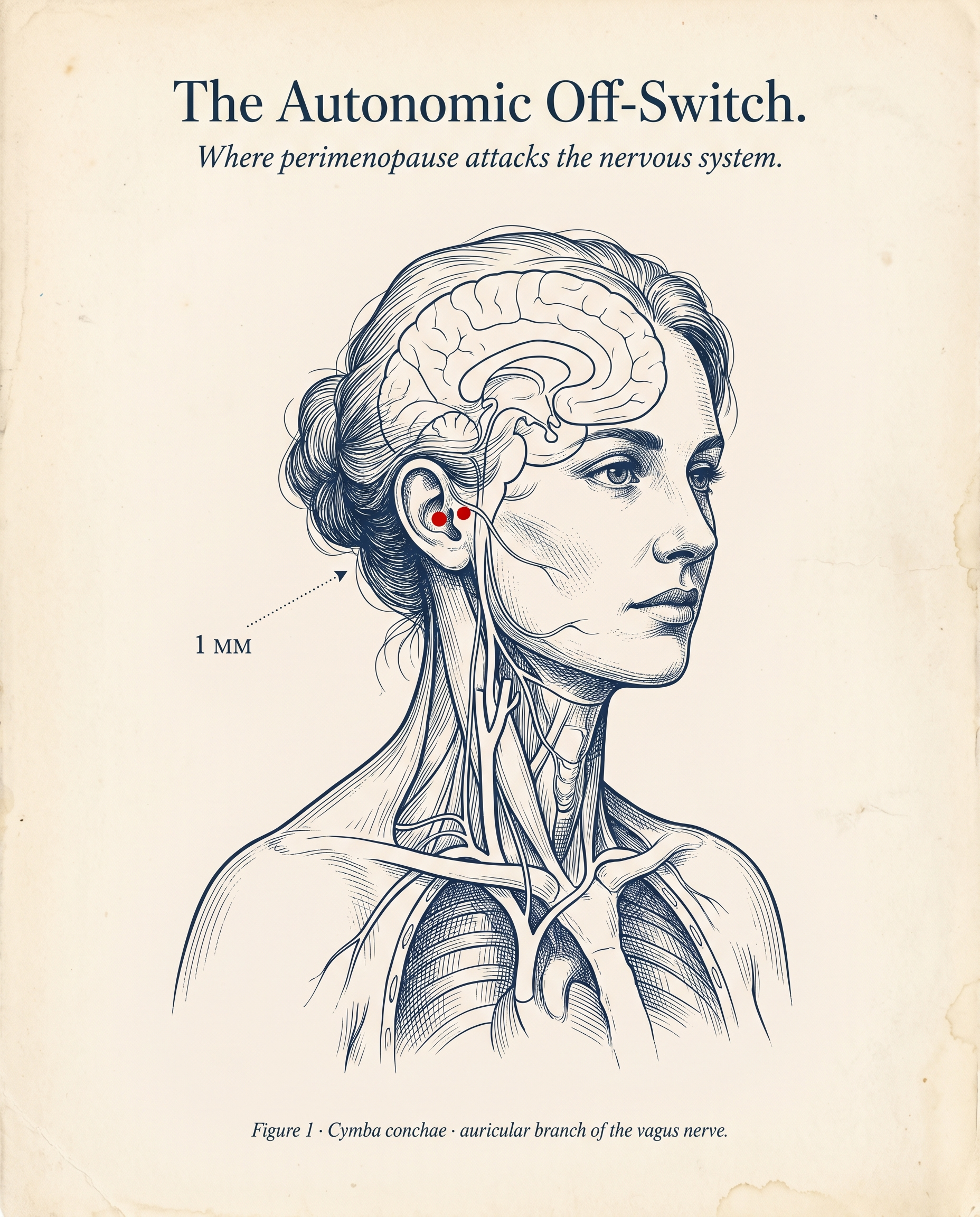
The vagus nerve runs that handoff. When estrogen falls, vagal tone weakens. The "off-switch" stops firing at the exact moment you need it.
This is why magnesium glycinate, L-threonate, taurate, melatonin, ashwagandha — and even HRT — leave the autonomic symptoms untouched for most women. They're aimed at the wrong layer.
"The intervention has to engage the autonomic system directly. Nothing in the supplement aisle does." Dr. K., Stanford autonomic medicine specialist (interviewed for this article)